HINTS+ Exam appears more sensitive than early MRI for detecting stroke in the first 24-48 hours. (Kattah 2009)
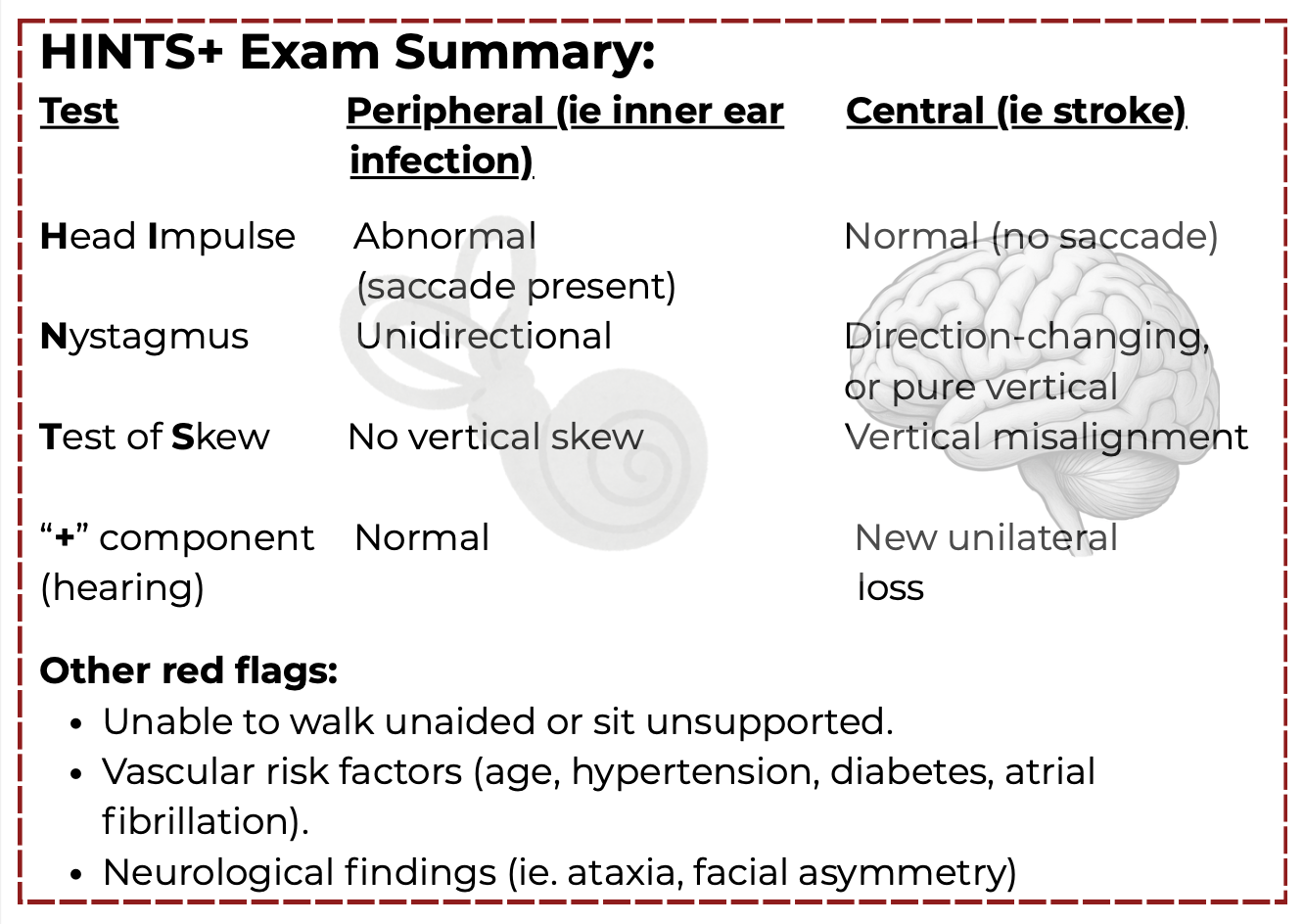
On the chart below note that only one central sign with a patient having acute vestibular syndrome = a central vestibular disorder (i.e. stroke) until proven otherwise.
When Should You Use HINTS+?
Use HINTS+ when a patient presents with Acute Vestibular Syndrome (AVS), characterized by:
1. Constant vertigo/dizziness
2. Nausea, vomiting
3. Spontaneous nystagmus
4. Gait instability
5. Head motion intolerance
How To Perform Each Test
Watch Real Examples of Abnormal Findings
INFARCT
Impulse
Normal,
Fast-phase
Alternating nystagmus,
Refixation
Cover Test (skew)
= stroke
SEND HIM HOME SAFE
Straight Eyes- No new Deafness
Head Impulses Misses
One-way Nystagmus
Healthy Otic & Mastoid Exam
Stand Alone & Face Even
= peripheral lesion
HINTS+ is a powerful tool when applied to the right patient, at the right time, by a trained examiner.
Don’t Miss a Stroke in Dizziness
Learn to use the HINTS+ exam to identify central and peripheral patterns in Acute Vestibular Syndrome in this FREE 1 hour training so you know when a patient is safe to treat and when escalation is required.
What You’ll Learn:
- When HINTS+ should and should not be used
- How to perform each component of the exam
- How to interpret findings as peripheral vs central patterns
- When findings require urgent escalation
- Key limitations and clinical pitfalls
✅ Course Certificate Included
✅ Lifetime Access
✅ Real Clinical Examples
Created by
Kregg Ochitwa, BScPT, CWCE, CredMDT, AVPT
Clinic Owner & Founder of North 49
Advanced Vestibular Physical Therapist
Labyrinthitis and vestibular neuritis:
These are two different inner ear conditions: vestibular neuritis (also known as acute unilateral vestibulopathy, or AUVP) and labyrinthitis. Both are typically viral in nature, with labyrinthitis also involving hearing loss. Both generally have a good prognosis, but evidence-based practice supports early referral to vestibular therapy to help maximize recovery. (Tokle 2020)
Labyrinthitis vs AICA Stroke:
- Labyrinthitis = inner ear infection + hearing loss
- AICA strokes can mimic labyrinthitis (peripheral signs plus hearing loss)
- With acute vestibular syndrome (AVS), if hearing loss is present, even with peripheral signs, serial testing and further investigation are warranted to rule out stroke.
Click on the TABLE below👇🏻 to download a more detailed flowchart for vestibular & non-vestibular causes of dizziness.

CONTACT INFO
(T) 306-343-7776
(F) 306-343-7780
(E) contactus@north49therapy.ca