Can Convergence Exercises Cause Harm After Concussion?

What the latest evidence says about Brock String therapy, convergence insufficiency, and spasm of the near reflex
A lot of us have been taught convergence exercises such as Brock String and pencil push-ups at courses related to concussion and vestibular rehabilitation.
Recently, however, concerns have emerged suggesting these exercises may worsen visual dysfunction or even cause permanent damage.
Given this, I thought it would be prudent to revisit the literature and see what the evidence actually says.
The short answer?
Current evidence does not support permanent structural visual or neurological harm from convergence exercises.
In fact, the newest concussion-specific research suggests that convergence exercises may be beneficial for appropriately selected patients recovering from concussion.
The more important question may not be whether convergence exercises are harmful, but rather:
Are we prescribing them to the right patient?
To answer that question, clinicians must understand the difference between two conditions that can sometimes look similar:
• Convergence Insufficiency (CI)
• Spasm of the Near Reflex
One often benefits from convergence exercises.
The other may worsen with excessive convergence loading.
Understanding the difference is critical.
Convergence Insufficiency Versus Spasm of the Near Reflex
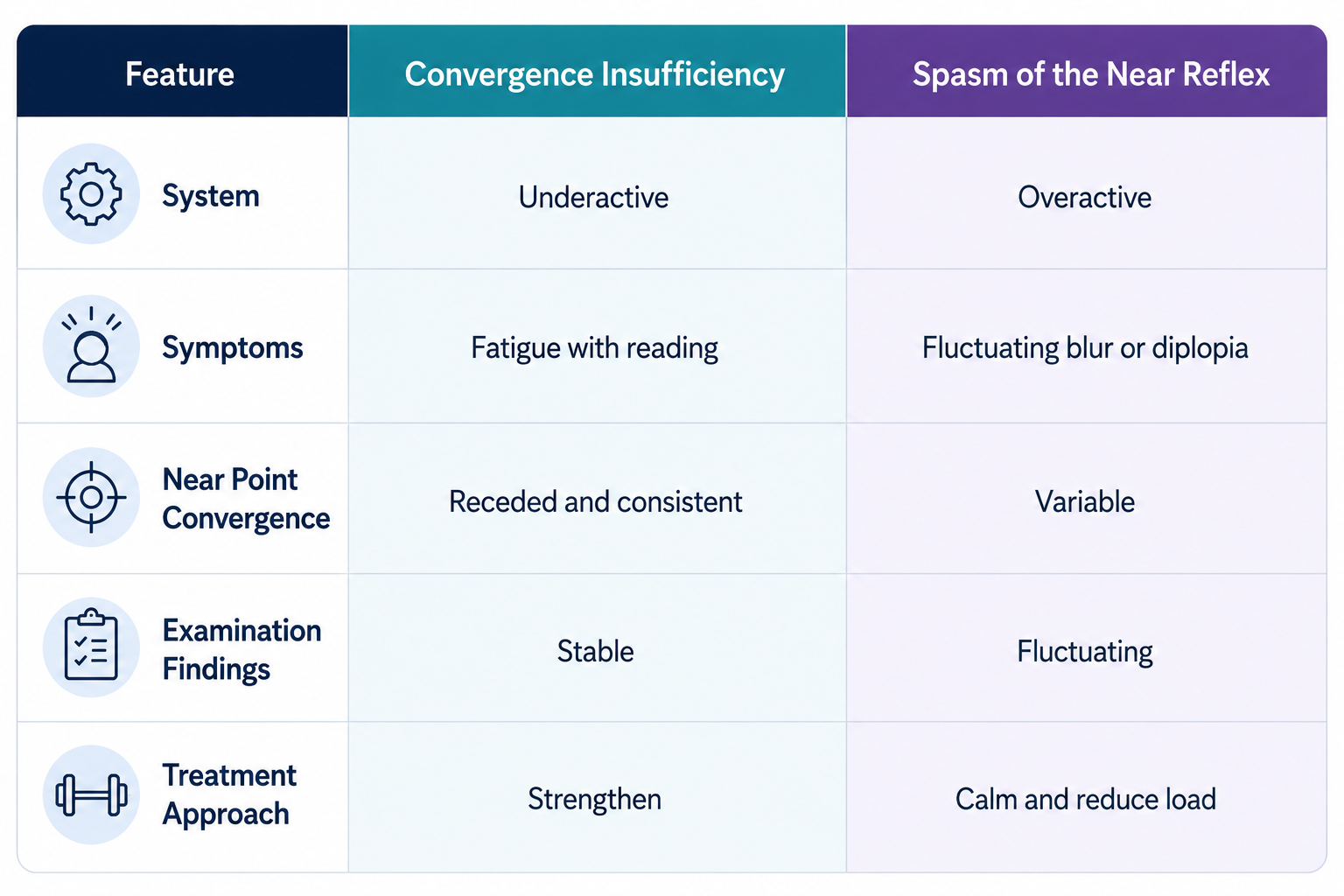
Convergence Insufficiency is essentially an underactive convergence system.
Patients struggle to bring and maintain their eyes inward when focusing on near targets.
Common complaints include:
• Eye strain with reading
• Headaches during near work
• Difficulty concentrating
• Symptoms that improve with breaks
• Fatigue during prolonged visual tasks
In contrast, Spasm of the Near Reflex represents an overactive system.
Rather than struggling to converge, the visual system may become stuck in an excessive near-focus state.
These patients may experience:
• Fluctuating blur
• Variable double vision
• Symptoms at both near and distance
• Inconsistent examination findings
• Episodic worsening that can be difficult to predict
While these conditions can appear similar at first glance, they often require very different treatment approaches.
The Clinical Clue Many Clinicians Miss
One of the most useful clinical clues is consistency.
Patients with true convergence insufficiency often demonstrate relatively stable findings. Their symptoms typically increase with visual demand and fatigue.
Patients with spasm of the near reflex frequently demonstrate variability. Near point convergence may change throughout an assessment. Symptoms may fluctuate dramatically between visits or even within the same session.
When findings are highly variable, clinicians should pause before automatically assuming convergence weakness.
Sometimes the issue is not a system that needs strengthening.
Sometimes it is a system that needs calming.
Can Convergence Exercises Cause Permanent Damage?
This is the question driving much of the recent discussion.
After reviewing the literature, there is currently no evidence that convergence exercises cause permanent structural visual or neurological injury.
To date, the literature has not demonstrated permanent structural injury when convergence exercises are prescribed to patients later suspected of having spasm of the near reflex.
That does not mean convergence exercises are always appropriate.
Exercises prescribed to the wrong patient may increase symptoms, worsen irritability, and create frustration.
However, worsening symptoms should not be confused with permanent injury.
The primary risk appears to be misapplication and sensitization rather than structural harm.
What Does the New Concussion Research Show?
Historically, much of the evidence supporting convergence therapy came from pediatric vision therapy literature and non-concussion populations.
That has started to change.
In 2025, Trbovich and colleagues published a randomized controlled trial investigating Brock String vision therapy in individuals aged 11 to 30 years who demonstrated a receded near point of convergence following concussion.
Participants were enrolled within approximately 10 days of injury and were assigned to either:
• Brock String therapy performed twice daily
or
• Usual care
The Brock String group demonstrated significantly greater improvements in near point of convergence compared to usual care, providing preliminary randomized controlled trial evidence that convergence rehabilitation can improve convergence performance following concussion.
These findings are important for several reasons.
First, they provide concussion-specific evidence supporting convergence rehabilitation.
Second, they suggest that appropriately selected patients may benefit from convergence exercises relatively early in recovery rather than waiting until symptoms become chronic.
Third, they provide evidence that convergence exercises can be beneficial following concussion when prescribed to appropriately selected patients.
However, it is important to recognize what the study actually investigated.
The researchers enrolled individuals with a receded near point of convergence consistent with convergence insufficiency.
The findings should not automatically be generalized to patients with suspected spasm of the near reflex, highly fluctuating visual findings, or highly irritable visual presentations.
Patient selection still matters.
When Convergence Exercises May Help
Convergence exercises may be beneficial when patients demonstrate findings consistent with true convergence insufficiency, including:
• Receded near point convergence
• Stable examination findings
• Fatigue-related symptoms
• Difficulty with sustained near work
• Reduced convergence endurance
Common convergence exercises include Brock String, pencil push-ups, and other graded convergence training approaches.
As with any rehabilitation program, dosage and progression should be individualized.
More exercise is not always better.
When Convergence Exercises May Not Be Appropriate
Clinicians should exercise caution when:
• Symptoms are highly irritable
• Findings fluctuate significantly
• Distance diplopia is present
• Near point convergence is inconsistent
• Symptoms worsen rapidly with minimal visual loading
In these situations, further assessment may be required before progressing convergence exercises.
Some patients may benefit more from strategies aimed at reducing visual load, calming autonomic arousal, improving exertional tolerance, addressing vestibular dysfunction, or managing migraine-related contributors before progressing to more intensive visual rehabilitation.
Clinical Takeaway
The discussion around convergence exercises is important, but it requires context.
Current evidence does not support permanent structural harm from appropriately prescribed convergence exercises.
Current evidence also does not demonstrate permanent structural injury when convergence exercises are prescribed to the wrong patient.
At the same time, emerging randomized controlled trial evidence suggests Brock String therapy can improve near point of convergence in appropriately selected patients following concussion and may be initiated as early as approximately 10 days post-injury.
As with most post-concussion interventions, exercise prescription should remain symptom-limited and individualized to patient tolerance.
The key is recognizing who is most likely to benefit.
Convergence insufficiency is a common and clinically meaningful finding following concussion.
Convergence exercises can absolutely help the right patient.
But not every convergence-related complaint represents weakness.
Some visual systems need strengthening.
Others need calming.
Our job as clinicians is determining which is which.
References
Cooper J, Jamal N. Convergence insufficiency—a major review. Optometry. 2012;83(4):137–158.
Author

Kregg Ochitwa
Physical Therapist I Vestibular Therapist I Clinic Owner
Categories
All Categories