Idiopathic Intracranial Hypertension: A Clinician's Guide to Diagnosis & Management
Every vestibular therapist has encountered the patient whose dizziness simply doesn't fit.
Vestibular testing is largely unremarkable, yet the patient reports persistent headaches, motion sensitivity, visual complaints, and imbalance. They may have already been diagnosed with vestibular migraine, Persistent Postural-Perceptual Dizziness (PPPD), cervicogenic dizziness, or even anxiety, but something about the presentation feels atypical.
One diagnosis that deserves a place on the differential is Idiopathic Intracranial Hypertension (IIH).
Although IIH is relatively uncommon, recognizing it is critically important because delayed diagnosis can result in permanent visual loss. As vestibular clinicians, we are often among the first healthcare professionals to evaluate these patients. While we are not responsible for diagnosing IIH, we are well positioned to recognize when a patient's presentation does not fit a peripheral vestibular disorder and facilitate appropriate medical referral.
The goal of this article is not to teach the neurological workup of IIH, but rather to help vestibular clinicians recognize the clinical features that should raise suspicion for this potentially vision-threatening condition.
What is Idiopathic Intracranial Hypertension?
Idiopathic Intracranial Hypertension (IIH) is a disorder characterized by elevated intracranial pressure (ICP) without an identifiable structural cause. Patients have increased pressure within the skull despite normal brain imaging, normal cerebrospinal fluid (CSF) composition, and no evidence of a mass lesion, hydrocephalus, or other secondary cause of raised intracranial pressure.
Although the exact mechanism remains incompletely understood, current evidence suggests the disorder is likely multifactorial. Proposed mechanisms include impaired cerebrospinal fluid absorption, abnormalities of cerebral venous drainage, hormonal influences, and metabolic factors that ultimately contribute to elevated intracranial pressure.
For vestibular clinicians, the underlying pathophysiology is less important than recognizing how elevated intracranial pressure produces symptoms that can closely resemble disorders we commonly assess in clinic.
How Common is IIH?
IIH is considered an uncommon condition, with an estimated annual incidence of approximately 1–3 per 100,000 peoplein the general population.
However, the incidence rises substantially in women of childbearing age with obesity, where rates may approach 20 per 100,000 people annually.
Although obesity remains the strongest recognized risk factor, clinicians should remember that IIH can also occur in:
- Men
- Children
- Adolescents
- Individuals with a normal body weight
Maintaining a broad differential diagnosis remains important, particularly when the clinical presentation raises concern.
Why Vestibular Clinicians Should Care
Many of the hallmark symptoms of IIH overlap with conditions commonly encountered in vestibular practice.
Patients frequently report:
- Dizziness
- Motion sensitivity
- Headaches
- Visual complaints
- Imbalance
Because of this, they often present first to:
- Vestibular physiotherapists
- Audiologists
- Otolaryngologists
- Specialized dizziness clinics
- General physiotherapists with an interest in vestibular rehabilitation
Before receiving the correct diagnosis, these patients may initially be labelled as having:
- Vestibular migraine
- Persistent Postural-Perceptual Dizziness (PPPD)
- Cervicogenic dizziness
- Anxiety-related dizziness
- Benign Paroxysmal Positional Vertigo (BPPV)
While these diagnoses are far more common than IIH, failing to recognize the clinical features that distinguish IIH can delay treatment and place the patient's vision at risk.
Fortunately, careful history taking and a targeted examination can often identify clues that the patient's symptoms do not fit more common vestibular conditions, prompting consideration of alternative diagnoses such as IIH.
Common Presenting Symptoms
Headache
Headache is the most common symptom of IIH and often reflects elevated intracranial pressure.
Patients commonly describe headaches that are:
- Daily or nearly daily
- Worse in the morning
- Worse when lying flat
- Aggravated by coughing, sneezing, bending, or straining (Valsalva)
- Severe enough to wake them from sleep
One important challenge is that many headaches associated with IIH closely resemble migraine, making differentiation difficult based on headache characteristics alone.
For this reason, vestibular clinicians should actively explore associated symptoms rather than relying solely on headache quality.
Visual Symptoms
Visual complaints often provide the most important clues that a patient's dizziness may not be vestibular in origin.
Patients may report:
- Blurred vision
- Double vision
- Reduced peripheral vision
- Difficulty focusing
- Brief episodes of visual dimming or vision loss
One symptom deserves particular attention:
Transient Visual Obscurations
Patients often describe these episodes by saying:
"My vision goes black for a few seconds."
These episodes typically last only a few seconds and frequently occur with standing, bending, or other positional changes.
Unlike a classic migraine aura, transient visual obscurations are thought to reflect elevated intracranial pressure affecting optic nerve function and should always prompt further questioning.
Pulsatile Tinnitus
Another highly characteristic symptom is pulsatile tinnitus.
Patients may say:
"I hear my heartbeat in my ear."
Unlike the continuous ringing commonly associated with sensorineural hearing loss, pulsatile tinnitus is typically described as a rhythmic "whooshing" sound synchronized with the heartbeat.
Although pulsatile tinnitus has multiple potential causes, its presence alongside headaches, visual symptoms, and dizziness should substantially increase suspicion for IIH.
Dizziness and Imbalance
Vestibular complaints in IIH are often nonspecific but can closely resemble conditions commonly encountered in vestibular practice.
Patients may report:
- Lightheadedness
- Motion sensitivity
- Persistent unsteadiness
- Difficulty walking in visually complex environments
- General disequilibrium
Unlike many peripheral vestibular disorders, dizziness is frequently accompanied by headaches, visual symptoms, or pulsatile tinnitus.
When significant dizziness occurs despite relatively normal vestibular findings, clinicians should broaden their differential diagnosis.
Red Flags During the Vestibular Assessment
Although IIH is uncommon, several clinical features should prompt vestibular clinicians to consider a non-peripheral cause of dizziness.
Maintain a higher index of suspicion when a patient presents with:
- Dizziness that appears disproportionate to vestibular examination findings
- Persistent headaches accompanying dizziness
- Transient visual obscurations
- Pulsatile tinnitus
- Headaches that worsen when lying flat
- Headaches aggravated by coughing, sneezing, or straining
- Binocular diplopia
- Papilledema
- An unexplained sixth cranial nerve palsy
No single finding confirms IIH. However, the combination of several of these features should prompt consideration of elevated intracranial pressure and appropriate medical referral.
How is IIH Diagnosed?
Idiopathic Intracranial Hypertension is a diagnosis of exclusion. No single symptom or examination finding confirms the diagnosis. Instead, specialists combine the patient's history, ophthalmologic examination, neuroimaging, and lumbar puncture findings.
The diagnostic workup typically includes:
- Fundoscopic examination to identify papilledema
- MRI of the brain with MR venography (or CT venography when appropriate) to exclude structural lesions and cerebral venous sinus thrombosis
- Lumbar puncture demonstrating an elevated opening pressure (generally >25 cm H₂O in adults) with normal cerebrospinal fluid composition
For vestibular clinicians, the important point is not memorizing the diagnostic criteria, but recognizing when a patient's presentation warrants referral for further medical assessment.
Clinical Questions That Should Raise Suspicion for IIH
One of the greatest strengths of vestibular clinicians is obtaining a detailed subjective history. A few targeted questions can quickly identify features that should broaden the differential diagnosis.
Consider IIH when a dizzy patient reports:
- "My vision briefly goes black."
- "I hear my heartbeat in my ear."
- "My headache is worse when I lie down."
- "My headache gets worse when I cough, sneeze, or strain."
- "My vision has gradually been getting worse."
- "The dizziness doesn't seem to match what you found during the examination."
While no single symptom confirms the diagnosis, the combination of headache, transient visual obscurations, pulsatile tinnitus, and relatively normal vestibular findings should significantly increase suspicion for elevated intracranial pressure and prompt appropriate medical referral.
Conditions That May Mimic IIH
Several disorders commonly encountered in vestibular practice share features with IIH. Appreciating both the similarities and the distinguishing characteristics can help guide clinical reasoning.
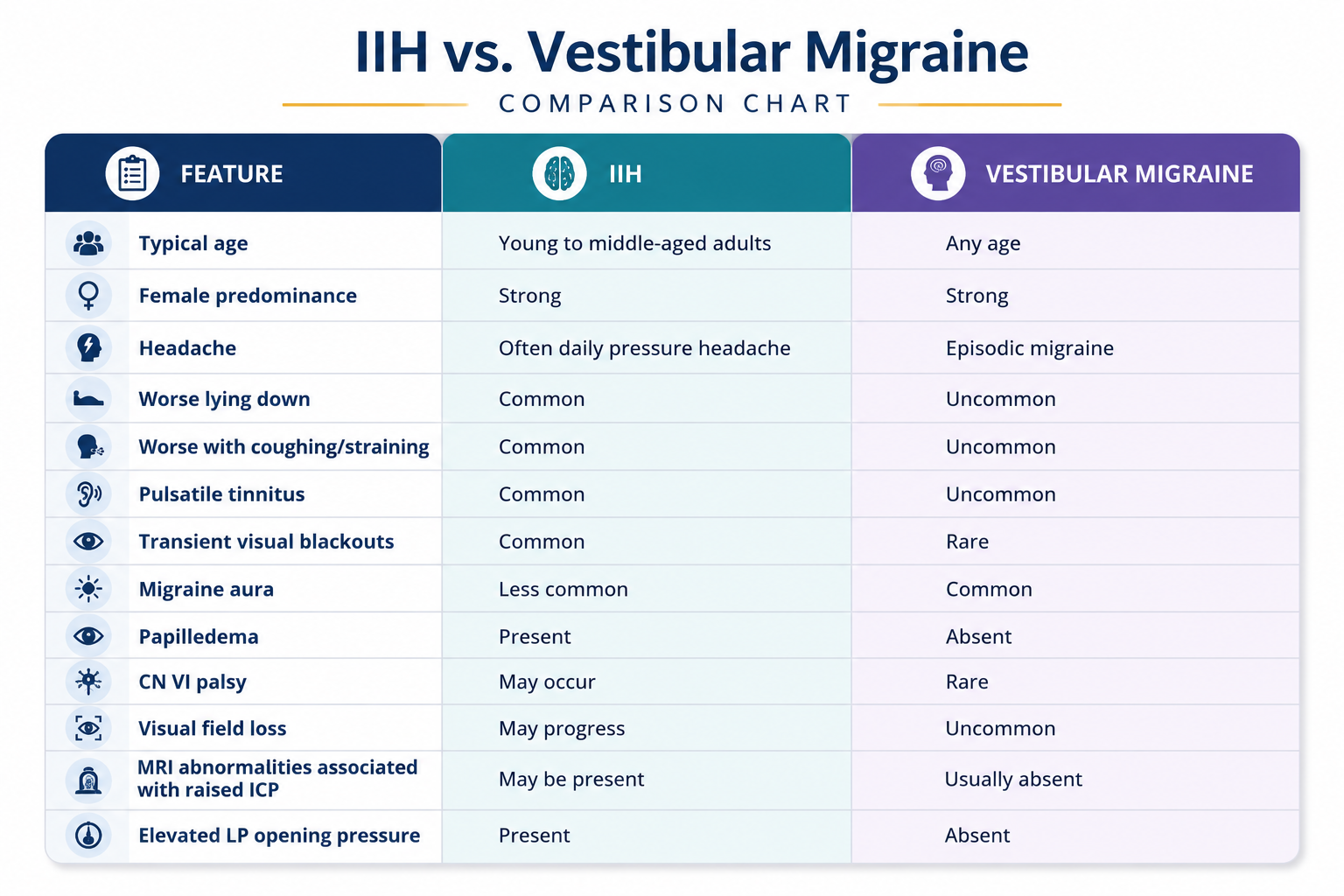
Vestibular Migraine
Vestibular migraine is probably the condition most likely to be confused with IIH because both can present with:
- Headaches
- Motion sensitivity
- Dizziness
- Visual complaints
However, transient visual obscurations, pulsatile tinnitus, papilledema, and headaches that worsen when lying flat or with Valsalva are not typical features of vestibular migraine and should prompt consideration of IIH.
Persistent Postural-Perceptual Dizziness (PPPD)
Patients with PPPD frequently report:
- Persistent dizziness
- Visual dependence
- Motion sensitivity
- Increased symptoms in visually busy environments
Unlike IIH, PPPD does not cause papilledema, pulsatile tinnitus, elevated intracranial pressure, or progressive visual loss.
Ménière's Disease
Some patients with IIH describe tinnitus, ear fullness, and dizziness, creating overlap with Ménière's disease.
However, fluctuating hearing loss and spontaneous episodes of vertigo remain the hallmark features of Ménière's disease, whereas headaches, papilledema, transient visual obscurations, and pulsatile tinnitus are much more suggestive of IIH.
Intracranial Mass Lesions
Brain tumours and other intracranial space-occupying lesions can also present with:
- Headaches
- Papilledema
- Visual disturbances
- Dizziness
This overlap highlights why neuroimaging is an essential part of the diagnostic workup whenever elevated intracranial pressure is suspected.
Treatment
The primary goals of treatment are to:
- Protect vision
- Reduce intracranial pressure
- Manage symptoms
Weight Management
For patients who are overweight, weight reduction remains one of the most effective interventions. Even modest weight loss has been shown to improve symptoms and reduce intracranial pressure.
Medication
Acetazolamide
Acetazolamide is considered the first-line medical treatment because it reduces cerebrospinal fluid production, helping lower intracranial pressure and preserve vision.
Topiramate
Topiramate may be particularly useful in patients with coexisting migraine features because it can reduce intracranial pressure while also providing migraine prophylaxis. It may also assist with weight loss in some patients.
Surgical Management
When vision is threatened or symptoms progress despite medical management, surgical intervention may be necessary.
Options include:
- Optic nerve sheath fenestration
- Cerebrospinal fluid shunting procedures
- Venous sinus stenting in carefully selected patients
Implications for Vestibular Rehabilitation
Vestibular rehabilitation is not a treatment for elevated intracranial pressure.
However, vestibular clinicians can play a critical role throughout a patient's care.
Our role includes:
- Recognizing clinical red flags.
- Identifying dizziness presentations that do not fit a peripheral vestibular disorder.
- Facilitating timely ophthalmologic or neurological referral.
- Managing secondary deconditioning once the patient is medically stable.
- Treating coexisting vestibular disorders, such as vestibular migraine, BPPV, or Persistent Postural-Perceptual Dizziness, when appropriate.
Importantly, some patients with IIH may also develop secondary motion sensitivity, visual dependence, or balance deficits after prolonged symptom duration. Once intracranial pressure has been appropriately managed, vestibular rehabilitation may help address these residual impairments and facilitate return to normal function.
For many patients, the most valuable intervention a vestibular therapist provides is not a vestibular exercise. It is recognizing that the clinical presentation warrants further medical investigation.
Case Example
A 34-year-old woman with a long-standing history of migraine was referred for vestibular rehabilitation after experiencing progressively worsening dizziness and motion sensitivity over the previous six months. Despite adjustments to her migraine management, her symptoms continued to worsen, and she was referred with a presumed diagnosis of vestibular migraine.
She described a constant feeling of unsteadiness that was aggravated by busy visual environments, grocery shopping, and rapid head movements. Her headaches had also become more frequent and she noted they were often worse when lying flat or when coughing.
Bedside vestibular assessment, including positional testing, head impulse testing, dynamic visual acuity, and oculomotor examination, was largely unremarkable. There was no evidence of BPPV or a peripheral vestibular hypofunction.
During the subjective examination, several additional details emerged. She reported that her vision would occasionally "go black for a few seconds" when bending over or standing up quickly. She also described hearing a rhythmic "whooshing" sound in both ears that matched her heartbeat. More recently, she had noticed intermittent blurred vision when reading or working on the computer.
Although none of these findings independently confirmed the diagnosis, together they suggested that the clinical presentation was no longer consistent with a typical vestibular migraine.
Because the combination of transient visual obscurations, pulsatile tinnitus, worsening headaches, and relatively normal vestibular findings raised concern for elevated intracranial pressure, she was referred back to her physician for further medical investigation. Ophthalmologic examination demonstrated papilledema, MRI with MR venography excluded secondary causes of raised intracranial pressure, and lumbar puncture confirmed an elevated opening pressure consistent with Idiopathic Intracranial Hypertension.
This case highlights an important lesson for vestibular clinicians: sometimes the greatest value of a vestibular assessment is not identifying a vestibular disorder, but in recognizing when the presentation no longer fits one.
Take-Home Points
- Include IIH in the differential diagnosis of patients presenting with dizziness, headaches, and visual complaints.
- Transient visual obscurations, pulsatile tinnitus, and headaches that worsen when lying flat or with Valsalva are particularly important clinical clues.
- Vestibular testing may be surprisingly normal despite significant symptoms.
- Papilledema is a medical red flag requiring prompt ophthalmologic or neurological assessment.
- Early recognition and appropriate referral may help prevent permanent visual loss.
Final Thoughts
As vestibular clinicians, we spend much of our careers recognizing patterns.
This article is not about memorizing another rare diagnosis. It is about recognizing when a patient's presentation falls outside the patterns we see every day.
When dizziness is accompanied by headaches, visual symptoms, pulsatile tinnitus, or surprisingly normal vestibular findings, pause before settling on a familiar diagnosis.
Sometimes the greatest value of a vestibular assessment is not identifying a vestibular disorder, but in recognizing when the patient needs something else.
References
Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome. Neurology. 2013.
Mollan SP, Aguiar M, Evison F, et al. The expanding burden of idiopathic intracranial hypertension. Eye. 2019.
Wall M. Idiopathic intracranial hypertension. Neurologic Clinics. 2010.
Markey KA, Mollan SP, Jensen RH, Sinclair AJ. Understanding idiopathic intracranial hypertension. Journal of Neurology, Neurosurgery & Psychiatry. 2016.
Mollan SP, Hoffmann J, Sinclair AJ. Advances in the understanding and management of idiopathic intracranial hypertension. Lancet Neurology. 2019.
Author

Kregg Ochitwa
Physical Therapist I Vestibular Therapist I Clinic Owner
Categories
All Categories